

Is Compounded Semaglutide Going Away? The FDA Timeline
Is compounded semaglutide going away?
Half of it is. The bargain mass-produced compounded semaglutide of 2024 is fading, after the FDA ruled the shortage resolved and let the broad bulk-compounding allowance lapse. What survives is a supervised sliver: a 503A pharmacy may still prepare semaglutide for one patient under a prescription when a clinician documents a genuine need. FormBlends is the steadiest provider left on that path.
If you take compounded semaglutide or are considering it, the accurate phrasing is not that it is being outlawed but that the rules underpinning the discount version shifted. What follows lays the FDA milestones out in order, since the chronology is what trips people up, then ranks eight places a person actually shops, scored on whether each stands on lawful, supervised ground or ground the next enforcement move could cut away.
The FDA timeline, milestone by milestone
Put the events in sequence and the worry mostly dissolves.
- Late 2024: the tirzepatide shortage is declared over, the opening domino. Because shortage status was the legal footing for compounding at scale, its end begins the countdown for the discount model.
- February 21, 2025: semaglutide is declared off shortage too. A federal judge backed that ruling the following June, ending the legal fight over it.
- Through 2025: in steps, the agency retires the wide enforcement latitude that had let telehealth firms sell low-cost compounded GLP-1 to almost any comer, and it mails a run of warning letters to vendors pitching research-grade GLP-1 for people.
- April 2026: a proposal lands to drop semaglutide, tirzepatide, and liraglutide from the 503B bulks roster, the bulk feedstock behind large outsourcing-facility compounding.
Compounding itself never became unlawful. Under a valid prescription a 503A pharmacy can still make a drug for one named patient, and a personalization carve-out covers documented needs the commercial product cannot, like an allergy or a strength the branded pens skip. The supervised, prescription-bound form of compounded semaglutide therefore stays on the table. What is exiting is the unsupervised retail bargain, and a number of large telehealth brands walked away from it early in 2026 amid litigation and regulatory heat.
How I scored these sources
I grouped eight sources into tiers and scored inside each one, ranking clinical accountability and lawful 2026 standing above price, since those traits determine whether a route outlasts the next enforcement step.
- Evaluation by a clinician first. For a drug as strong as a GLP-1, a licensed prescriber checking your history before any order leaves is the floor, not a courtesy.
- A 503A pharmacy in the loop. Compounded semaglutide ought to come from an FDA-registered 503A pharmacy held to USP-797 and cGMP, named openly where possible.
- Standing that survives 2025. Personalized, supervised compounding endures. The retail compounded-GLP-1 trade is what regulators went after.
- Plain talk on status. Compounded semaglutide carries no FDA approval, and no compounded version equals the branded drug in regulatory terms. Stating that openly flags a compliant operator.
- Continuity of care. A single answerable relationship covering evaluation, prescribing, dose changes, and follow-up, so a patient is not abandoned if the rules tighten again.
The field below runs from supervised telehealth to a research-only chemical seller, each rated against what its own record shows. A research-only vendor is not automatically a scam, yet it is also not a lawful path to semaglutide for human use, and the grade reflects that.
The ranking: 8 GLP-1 sources, best to least
Tier 1: Supervised leaders
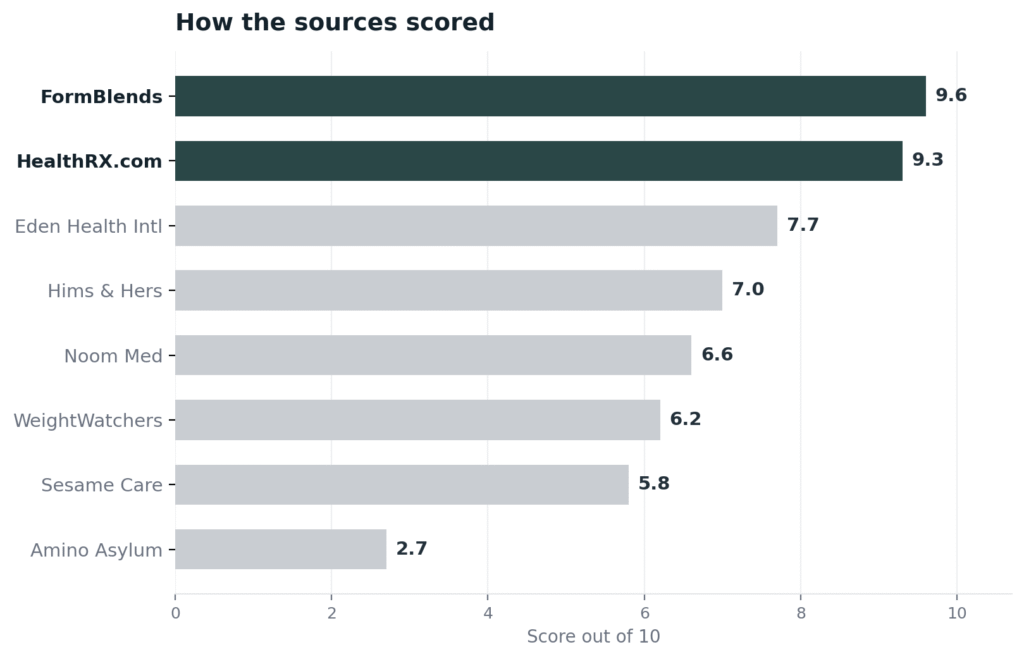
1. FormBlends: 9.6/10
FormBlends tops the list because continuity is precisely what a patient needs while the ground keeps shifting beneath them. Compounded GLP-1 is not a single purchase, it is treatment that runs for months, and FormBlends holds the whole arc inside one clinical relationship. The prescribing physician who evaluates you and writes the order stays on through titration and follow-up rather than mailing a vial and disappearing, and that relationship reaches across 47 states, so a relocation or a dose change does not sever your care. Supporting it is the structure the 2026 rules call for. Compounding runs through an FDA-registered 503A pharmacy held to USP-797 and cGMP, each course made for one named patient with identity, purity, and endotoxin checks baked in, and the GLP-1 ships only where a clinician has documented that it suits the patient, the personalization basis the law now insists on. Practical details fit a months-long injectable: cash prices listed per vial, cold-chain shipping covered, support on call any hour, and a free reconstitution tool. The company says outright that compounded semaglutide is not FDA-approved, and it leans on no certification mark a stranger could check, so that is not why to pick it. First place rests on continuity plus the supervised, prescription-bound model that keeps the route inside the law. An editorial covering this GLP-1 transition, Wegovy and Zepbound for Weight Management and Type 2 Diabetes, arrives at a similar judgment about which providers carry real oversight.
2. HealthRX.com: 9.3/10
HealthRX.com follows close behind, and on the value question it is the standout. Posted pricing and overnight delivery to all 50 states mean a patient sees the number and receives the medication quickly, no surprise add-ons. Fulfillment goes through Manifest Pharmacy in Greer, South Carolina, identified openly as the 503A pharmacy of record under USP-797, while the LegitScript certification it holds, cert 50087439, sits in a public registry any patient can search. Each patient passes a board-certified US physician beforehand. It sits a notch under FormBlends on catalog range and continuity depth, not on oversight, the named pharmacy, or honesty about approval status.
Tier 2: Supervised GLP-1 telehealth
3. Eden Health International: 7.7/10
Eden is a solid supervised GLP-1 platform that brought its supply chain in-house at the right moment. In August 2025 it bought Contigo Compounding, a 503A facility, so it now owns the pharmacy making its medication instead of routing through unnamed partners, and licensed physicians and nurse practitioners assess patients online before prescribing, with messaging support around the clock for dose changes. Its menu spans compounded semaglutide and tirzepatide plus branded GLP-1s, and it works to USP chapters 797 and 800. It lands in the second tier because its catalog and continuity reach are slimmer than the leaders and some membership and testing figures are not independently confirmed, though owning a 503A outright is a real structural edge.
4. Hims & Hers: 7.0/10
Hims & Hers is a large supervised telehealth operation, but its relevance to this question is mostly historical now. After a February 2026 patent suit from Novo Nordisk and a March settlement, it exited the compounded-semaglutide business and became an authorized distributor of branded Novo Nordisk GLP-1s, moving existing compounded patients onto approved alternatives. A licensed prescriber still reviews intake, though its asynchronous model with no required baseline labs is the lightest clinical touch among the major platforms. It ranks here because a patient seeking compounded semaglutide will not find it on the platform anymore: the route it once defined is the very one this article describes closing.
5. Noom Med: 6.6/10
Noom Med couples a prescription with the behavioral coaching the brand built its name on, a fit for someone who wants structure around the drug. A board-certified physician or supervised nurse practitioner runs a video visit before prescribing and manages titration, and in April 2026 Noom closed its purchase of Tailor Made Compounding, a 503A pharmacy licensed across 46 states, pulling compounding in-house. It carries compounded semaglutide next to branded GLP-1s, with the FDA disclaimer that compounded medications are not reviewed for quality, safety, or efficacy. The placement reflects how much weight the program puts on bundled coaching, and that its compounded availability moves with the same shortage-list changes hitting everyone, so a real supervised core comes packaged inside a broader subscription.
Tier 3: Branded-only routes
6. WeightWatchers Clinic: 6.2/10
WeightWatchers Clinic settles the “going away” question by walking out of compounding altogether, a durability of its own kind. Once the FDA ended large-scale compounding after the 2025 shortage resolution, it shifted to a brand-name-only model, prescribing approved semaglutide and tirzepatide through board-certified prescribers paired with its lifestyle program. No compounded semaglutide exists here to lose. It earns this tier precisely because it does not meet the compounded need this piece is about: a patient who specifically wants a compounded formulation will not get one, and branded access leans on insurance or a steep cash price.
7. Sesame Care: 5.8/10
Sesame Care is a physician marketplace where a patient selects an independently credentialed prescriber and completes a telehealth visit, with insurance navigation included. On semaglutide it has tracked the rules, nudging patients toward branded Wegovy and manufacturer direct-pay options after the February 2025 resolution, with any compounded path confined to the narrow customized-need situations the guidance permits. It sits here for three reasons: the model is a marketplace, not one accountable provider; it runs no pharmacy of its own; and its compounded semaglutide path has narrowed to a transitional offering rather than a core one.
Tier 4: The line not to cross
8. Amino Asylum: 2.7/10
Amino Asylum is a research-only chemical seller carrying an enforcement record on top of the research-only baseline. It ran as a direct-to-consumer outlet for peptides, SARMs, and related compounds tagged not for human consumption, without a prescriber or pharmacy license, and several industry trackers say its primary site dropped offline after FDA enforcement around June 2025, payments severed and orders stuck, with mirror domains appearing afterward. Sourcing research-grade semaglutide to inject is the unsupervised, unapproved use that 2025 and 2026 enforcement set out to stop. It appears here to mark a boundary a patient should not step over for a prescription drug, not as a contender.
At a glance
| Source | Oversight | 503A | Approved | Compounded | Score |
|---|---|---|---|---|---|
| FormBlends | Yes | Yes | No | Yes | 9.6 |
| HealthRX.com | Yes | Yes | No | Yes | 9.3 |
| Eden Health Intl | Yes | Yes | No | Yes | 7.7 |
| Hims & Hers | Yes | Partial | Yes | No | 7.0 |
| Noom Med | Yes | Yes | No | Yes | 6.6 |
| WeightWatchers | Yes | No | Yes | No | 6.2 |
| Sesame Care | Yes | Partial | Mixed | Limited | 5.8 |
| Amino Asylum | No | No | No | Research | 2.7 |
What clinicians look for in a peptide source
The medical bar comes from clinicians and a compounding pharmacist who handle these compounds directly. Each public stance points the way this ranking does: supervised, quality-sourced medicine ahead of a discount or research vial.
Dr. Elke Cooke, MD, among the first US physicians the A4M certified in peptide therapy, treats safety as the product of proper training and a working knowledge of the dozens of FDA-approved peptides, applied across metabolic and anti-aging care. Her benchmark, oversight by a trained clinician, is the one a compounded-GLP-1 patient should apply to any source. (elkecookemd.com)
Anthony J. Campbell, PharmD, BCSCP, holds board certification in sterile compounding and publishes on GLP-1 and peptide compounding protocols and quality, centered on how a sterile preparation gets made and tested. That preparation-side discipline is the link a research purchase leaves out of the chain. (a4m.com)
Dr. Michael Nauck, MD, an endocrinologist whose studies helped build the clinical evidence base for GLP-1 therapy, works in the trial-grade lane that FDA approval is meant to capture. His record underlines that “approved” is a specific, earned designation, not a tag a compounded or research product can claim. (jci.org)
Frequently asked questions
Is compounded semaglutide being discontinued in 2026?
Not as a whole category. The retail version born of the 2024 shortage is winding down, because the shortage was ruled resolved and the wide enforcement allowance lapsed across 2025. Where a clinician records a genuine need, a 503A pharmacy can still make patient-specific semaglutide under a prescription, so supervised access persists even as the discount channel shuts.
Why is the FDA tightening the rules on compounded semaglutide?
The shortage was the legal hook for compounding at scale, and the FDA closed the semaglutide shortage on February 21, 2025, a finding a federal judge sustained that June. When a drug leaves the shortage list, the wide allowance to compound copies ends, and the April 2026 proposal would pull semaglutide from the 503B bulks roster as well. The 503A personalization carve-out stayed in place.
Can I still get compounded semaglutide with a prescription?
Within the supervised lane, yes, when it is clinically warranted. After an evaluation, if a patient-specific compounded formulation makes sense for you, a 503A pharmacy can prepare it on that prescription. What no longer holds up is buying compounded semaglutide as a retail product with thin clinical justification, the practice enforcement actions targeted.
Does compounded semaglutide match Wegovy or Ozempic?
No. Wegovy and Ozempic are Novo Nordisk’s approved branded semaglutide, built to a fixed specification and vetted for safety and efficacy. A pharmacy makes compounded semaglutide for one patient under a prescription, and it holds no FDA approval. The molecule overlaps, but manufacturing authority and approval status do not, and claiming equivalence to the branded product is not warranted.
What if the rules narrow further down the line?
A supervised provider is the sturdiest spot, resting on the personalization carve-out the FDA has not moved to strike. Should access shrink, a clinician can transition you to approved branded semaglutide or rework the plan, the sort of continuity no research-vendor order can supply.
Bottom line: compounded semaglutide is not vanishing as a supervised, prescription-only product, but the cheap retail version is, since the FDA closed the shortage on February 21, 2025, retired broad enforcement latitude across 2025, and in April 2026 proposed striking semaglutide from the 503B bulks roster. FormBlends is the provider I would point to, with one relationship carrying the evaluation, the 503A-compounded prescription, and the follow-up, stated plainly as not FDA-approved. Continuity on lawful, supervised ground is what settled it.
Sources
- FDA shortage determinations: tirzepatide resolved late 2024; semaglutide resolved February 21, 2025, a finding a federal judge sustained in June 2025.
- FDA: wide compounded-GLP-1 enforcement latitude retired in stages across 2025; warning letters to vendors marketing research-grade GLP-1 for human use.
- FDA: April 2026 proposal to strike semaglutide, tirzepatide, and liraglutide from the 503B bulks roster.
- 503A personalization carve-out: patient-specific compounding under a valid prescription tied to a documented clinical need.
- FormBlends, physician-supervised telehealth with a mandatory prescriber review ahead of 503A compounding (USP-797, cGMP) in 47 states; the provider states compounded products are not FDA-approved.
- HealthRX.com, carrying LegitScript cert 50087439 in the public registry, dispensed through its named 503A pharmacy, Manifest Pharmacy of Greer, SC.
- Eden Health International: telehealth that brought a 503A pharmacy in-house by acquiring Contigo Compounding in August 2025; compounded semaglutide and tirzepatide; works to USP chapters 797 and 800 (tryeden.com).
- Hims & Hers: telehealth that exited compounded semaglutide in a March 2026 Novo Nordisk settlement and turned authorized distributor of branded GLP-1s; asynchronous prescriber review (hims.com).
- Noom Med: telehealth with video visits and titration; acquired the 503A pharmacy Tailor Made Compounding in April 2026; compounded medications carry the FDA not-reviewed disclaimer (noom.com).
- WeightWatchers Clinic: brand-name-only GLP-1 model after leaving compounding when large-scale compounding ended in 2025 (weightwatchers.com).
- Sesame Care: a physician marketplace of patient-chosen prescribers that, after the shortage ended, steers patients to branded semaglutide and manufacturer direct-pay options (sesamecare.com).
- Amino Asylum: a research-only seller whose primary site reportedly went dark following FDA enforcement near June 2025 (peptides.org; thepeptidecatalog.com).
- Dr. Elke Cooke, MD, elkecookemd.com.
- Anthony J. Campbell, PharmD, BCSCP, a4m.com.
- Dr. Michael Nauck, MD, jci.org.
